



Hi! - ENG




Os compartimos diferentes consejos clínicos para tratar grandes atrofias maxilares a partir de un caso clínico cedido por los Drs. Javier Herce, Álvaro Tofé y Martín Toledo.
An indispensable requirement when rehabilitating a patient with bone implants and achieving predictability is to have an adequate bone volume. However, in daily clinical practice it is common to find patients with insufficient alveolar ridges, large bone defects or atrophies that will require reconstructive bone augmentation techniques prior to or simultaneously with implant placement.
In cases where there is no residual alveolar ridge in the maxilla, which makes the placement of conventional endosseous implants impossible, and conventional bone regeneration or reconstruction techniques are not indicated or are not very predictable, Customized Subperiosteal Implants (ISP) are a good alternative to zygomatic implants since they will allow passively joining a fixed dental rehabilitation to its connections, with an optimal distribution of the prosthetic load, to restore functionality and esthetics to the patient.
ISPs are custom-made medical devices designed according to the medical prescription of a clinician and manufactured in a facility that has a license for the manufacture of custom-made medical devices and a quality management system according to ISO13485.
The regulation applicable to this type of products is the MDR (EU) 2017/745 regulation and the Spanish Royal Decree RD 192/2023 and therefore they must always be accompanied by their corresponding declaration of conformity indicating compliance with the general safety and performance requirements of this regulation.
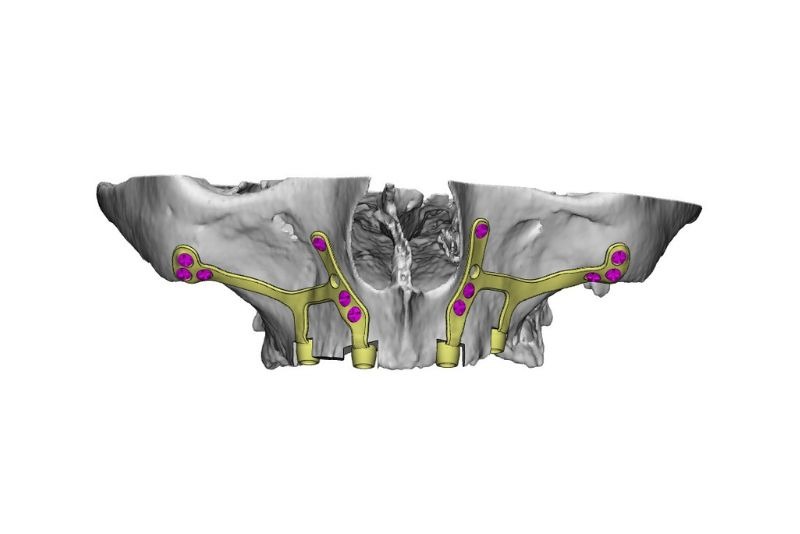
In order to design an ISP, radiological imaging of the patient’s bone and the position of the dental prosthesis in the mouth is necessary. For this it is essential that this image is a helical CT, since the use of lower quality images such as a CBCT can give rise to erroneous data that will interfere in the precise adjustment of the implant. From this information it will be possible to design the implant, plan the fixation areas and prosthetic connections according to the patient’s gingival level.
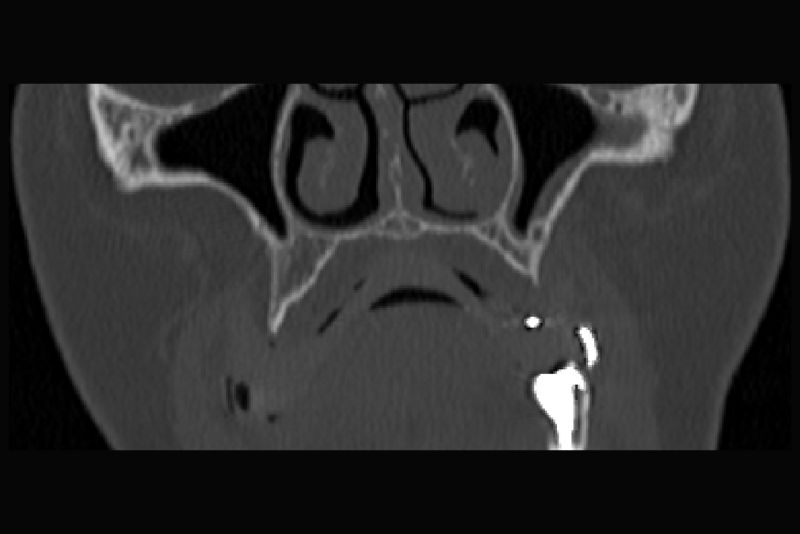
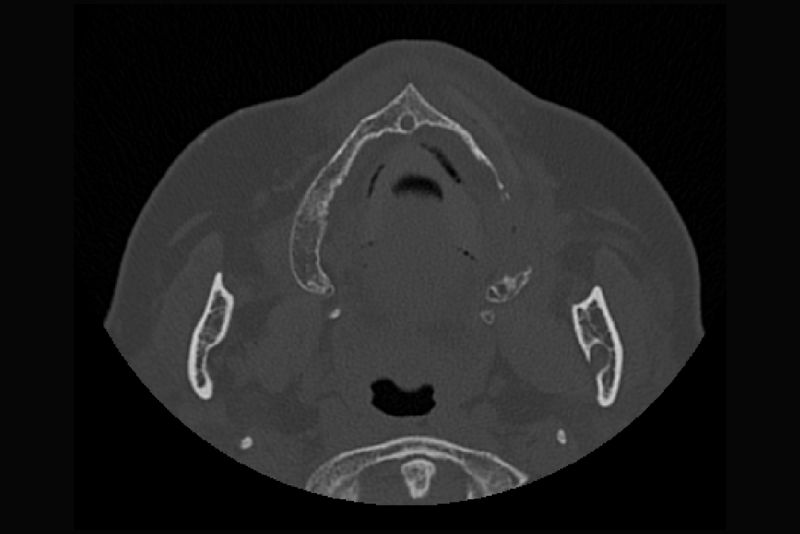
The implant is designed according to the atrophy and, in cases where there are alveolar bone remains and/or bone irregularities in the atrophy, it is essential to remove them by means of a cutting guide. In this way the implant is completely supported in the basal bone, avoiding the risk of mobility and avoiding possible dehiscence in the soft tissue with exposure of the implant to the oral environment.
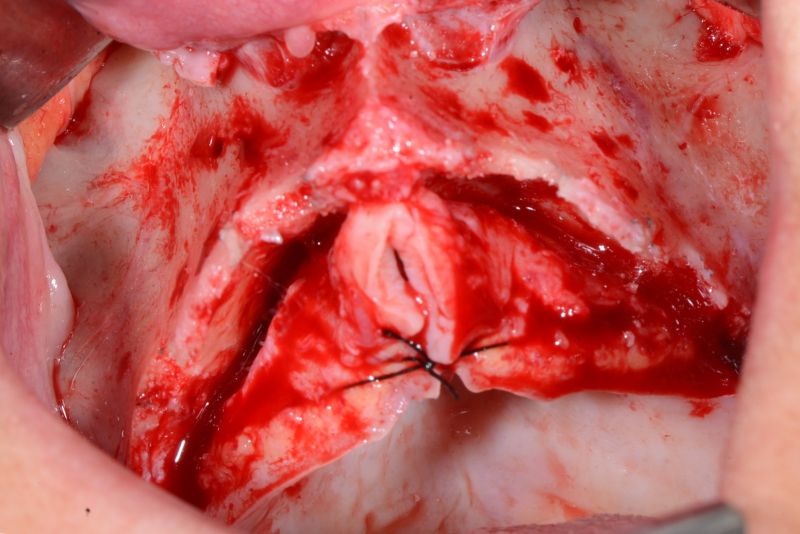
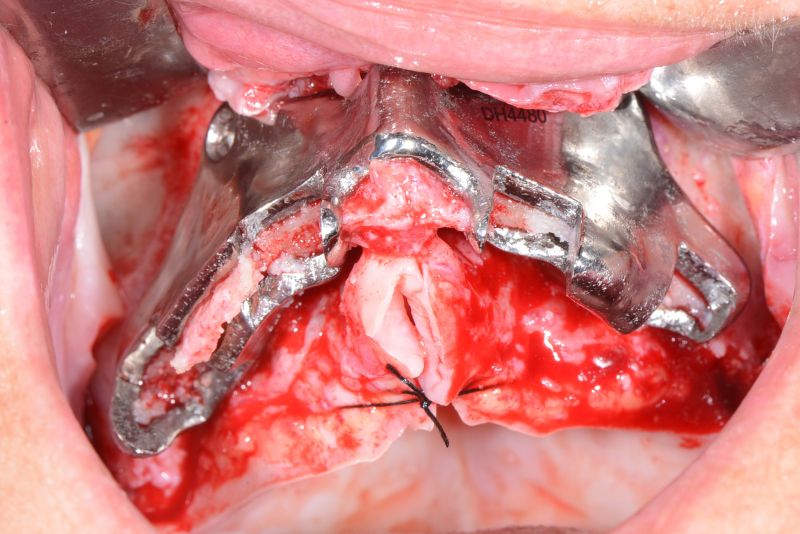

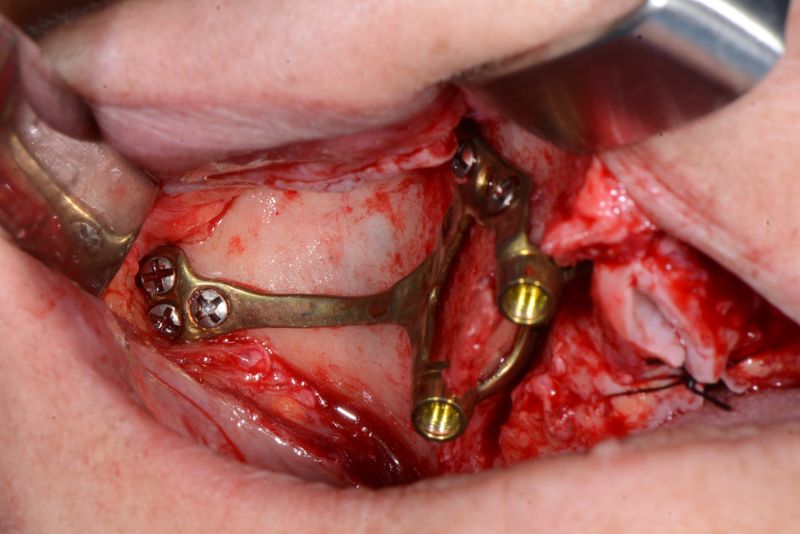
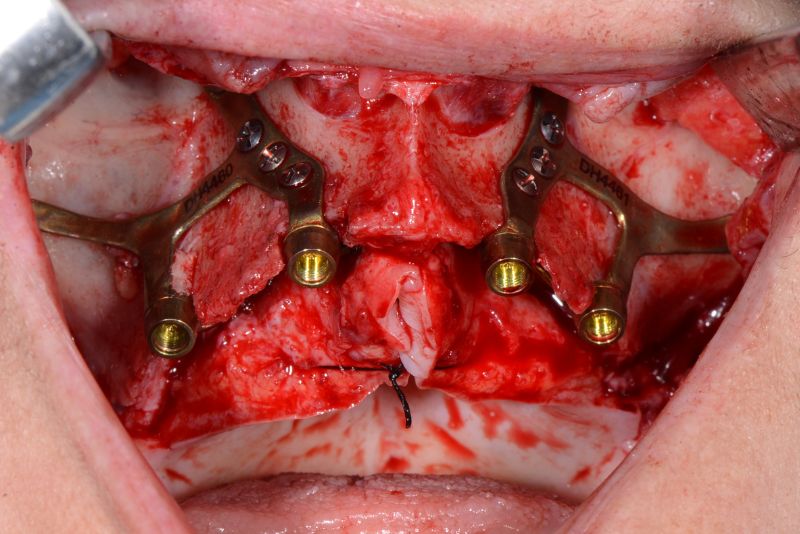
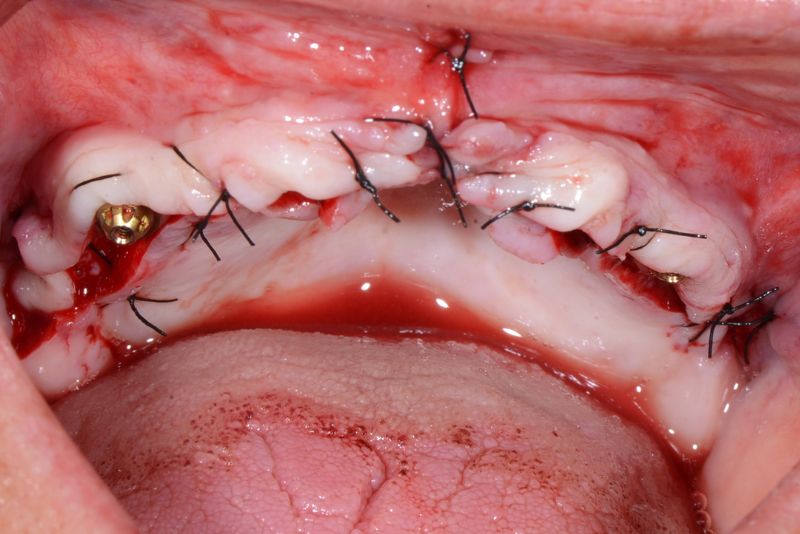
The design of the specific transepithelial abutments for ISP allows the prosthesis connection to be moved to the paragingival level, restoring the biological width and achieving optimal tissue sealing.
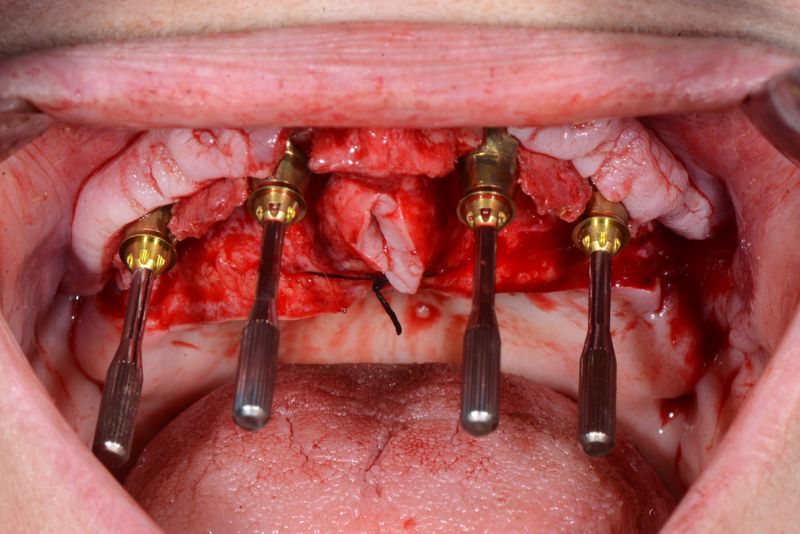
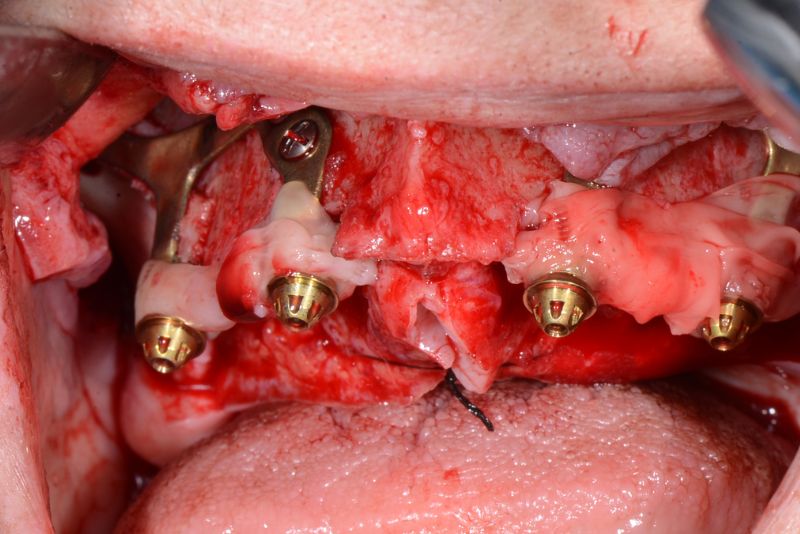
These interfaces, with different heights, guarantee the passive adjustment of the screw-retained prosthesis from the moment of surgery in immediate loading procedures. The convergent design without edges of the abutments guarantees the continuity of the connection, favoring the vascularization of the tissue and the adaptation of the mucosa for good maintenance and long-term stability.
Learn about the main features of Avinent’s transepithelial abutments for ISP.

Thanks to the large number of cases performed by maxillofacial surgeons Javier Herce and Álvaro Tofé, clinical data on the use of Customized Subperiosteal Implants for the treatment of severe maxillary atrophies are now available and their experience allows them to suggest the following recommendations.
If you want more information about Customized Superiosteal Implants you can access the scientific publication that was extracted from the ISP Consensus held in our facilities.
We are available to help you solve all your clinical challenges, contact us to get started!