Hi! - ENG




Ver evolución gráfica del caso
To avoid risking the esthetic and functional results of the implant-supported restoration, we must start with satisfactory bone volume, which allows the implants to be inserted with the restoration, and not the available bone, guiding us in three dimensions. However, in day-to-day clinical practice we sometimes come across situations of atrophy that are going to require an increase in the alveolar ridge to be able to proceed with implant insertion. Or the use of bone regeneration simultaneous to implant placement to treat fenestrations and dehiscence resulting from drilling these atrophic crests.
As shown below in this clinical case, the current guided bone regeneration (GBR) techniques are an excellent alternative for obtaining good esthetic results in the regeneration of periimplant defects.
Patient aged 58 years, non-smoker, with allergy to Enantyum and effervescent medicines being the only aspects of interest in her medical history, consulted the clinic to replace her lower removable prosthesis she used due to various absent teeth in the anterior sector, third and fourth quadrants, with a fixed restoration.
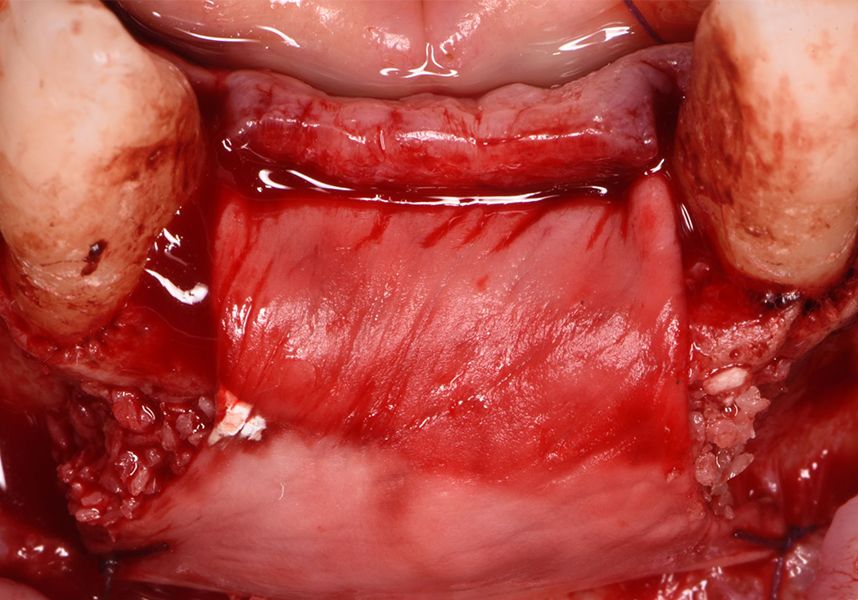
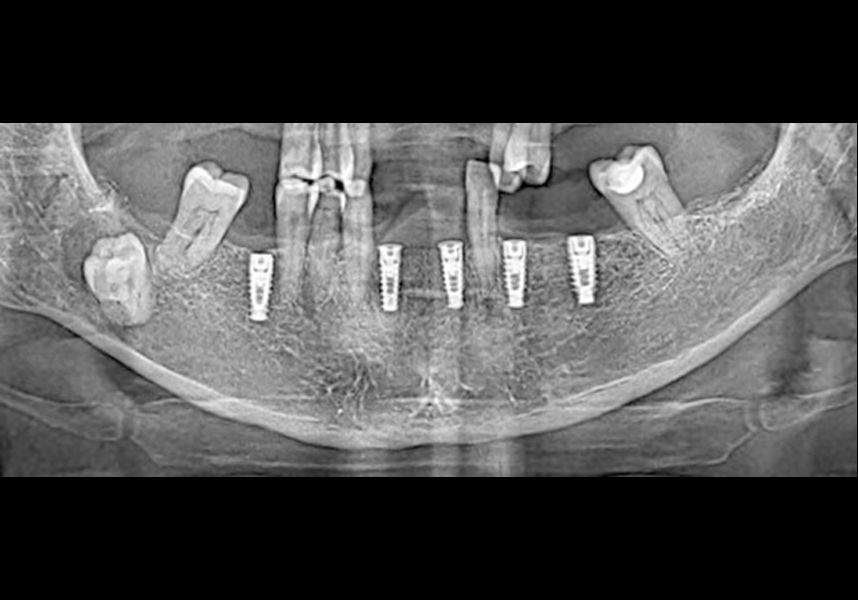
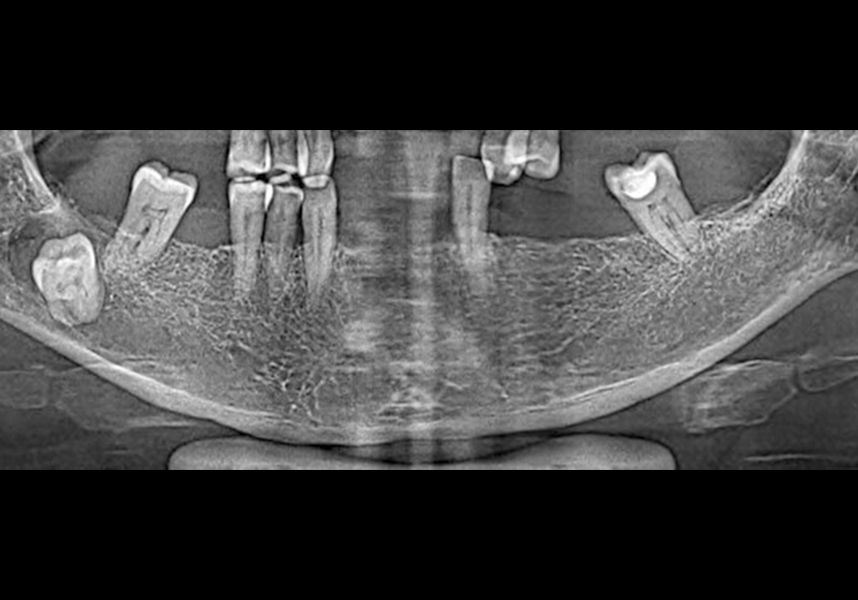
In the initial intraoral examination we observed an alveolar ridge that was optimum at coronal level, but with presence of significant bone concavity in the apical at anteroinferior level.
Placement of two dental implants was considered in the anteroinferior area, with simultaneous guided bone regeneration during the same surgery and the subsequent delayed placement of a metal-ceramic bridge for four teeth from 42 to 32. In addition, it was planned to insert three implants in positions 46, 34 and 36, also for restoration with metal-ceramic prosthesis.
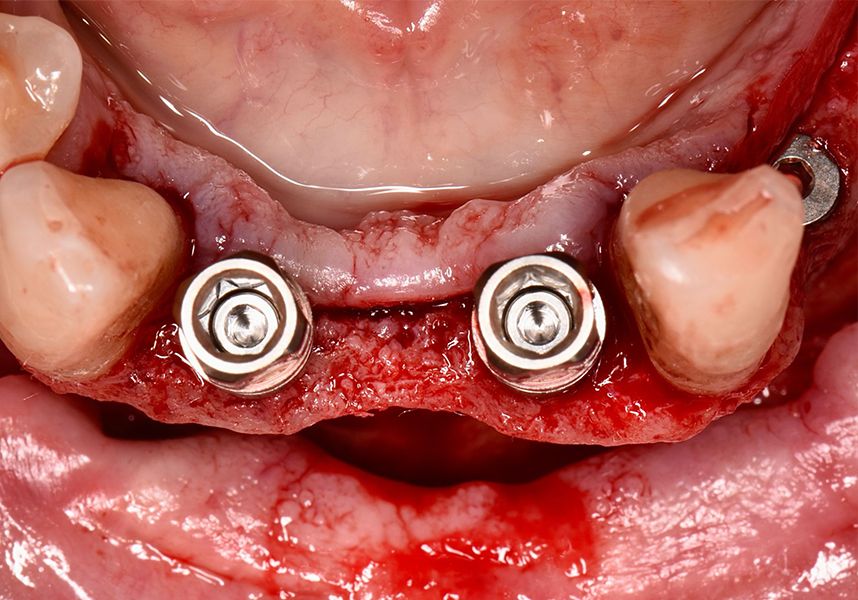
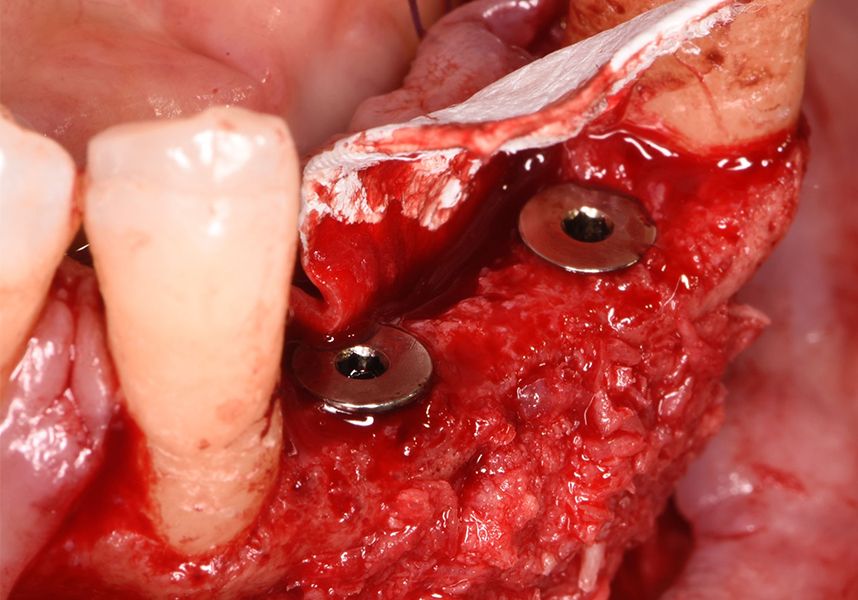
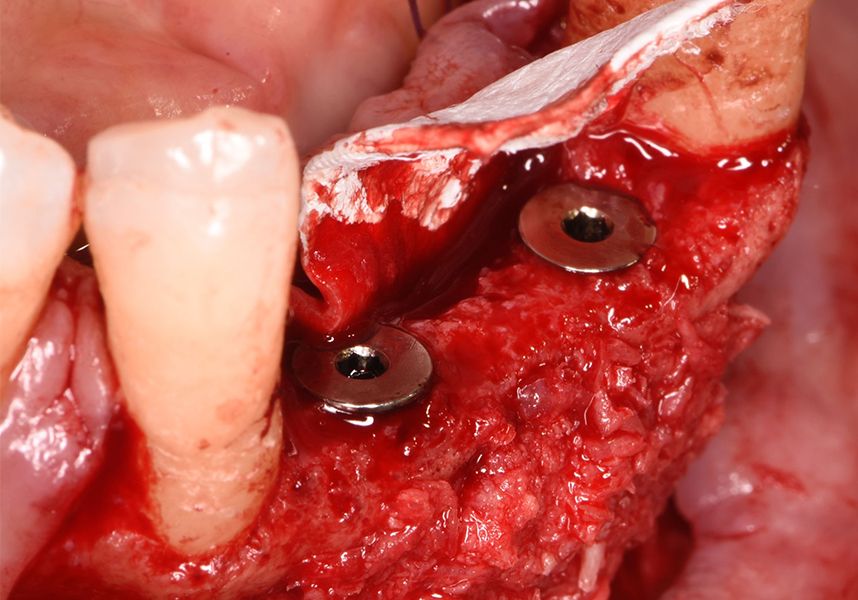
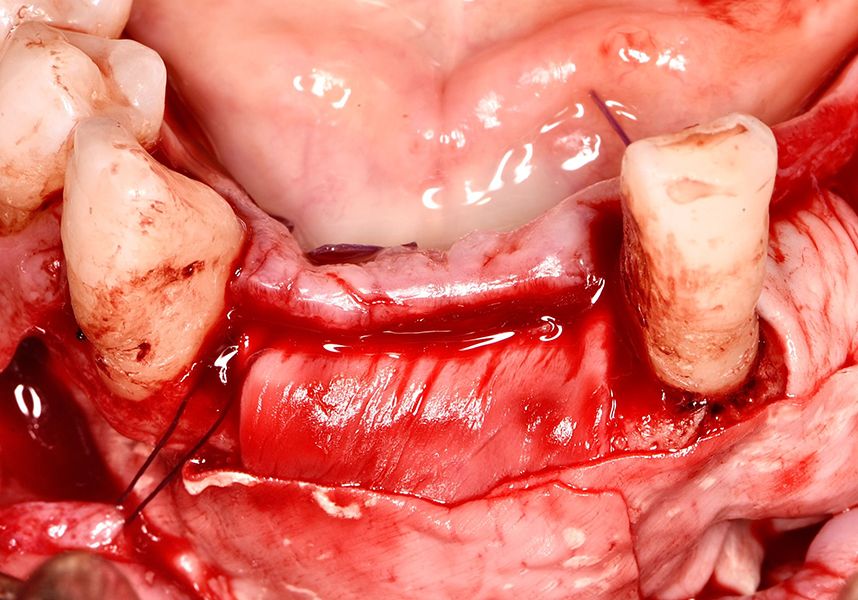
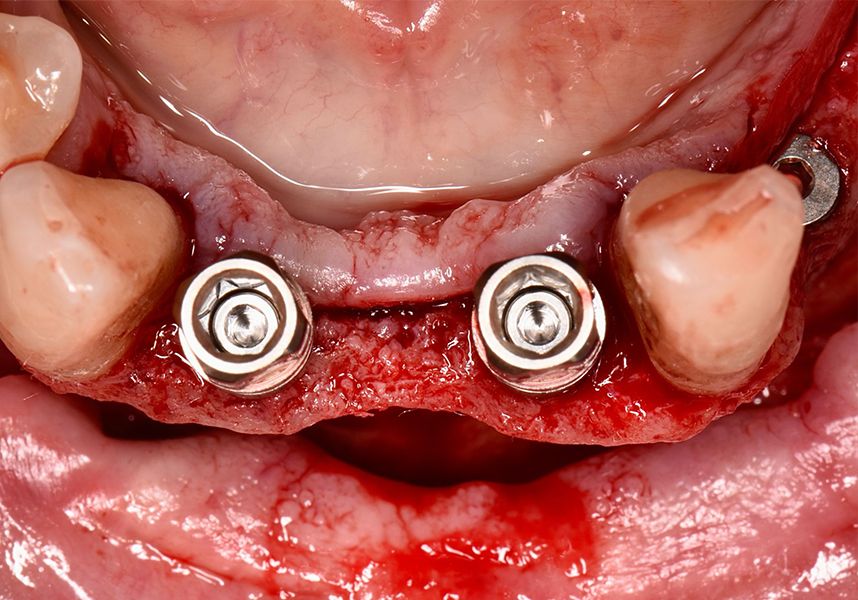
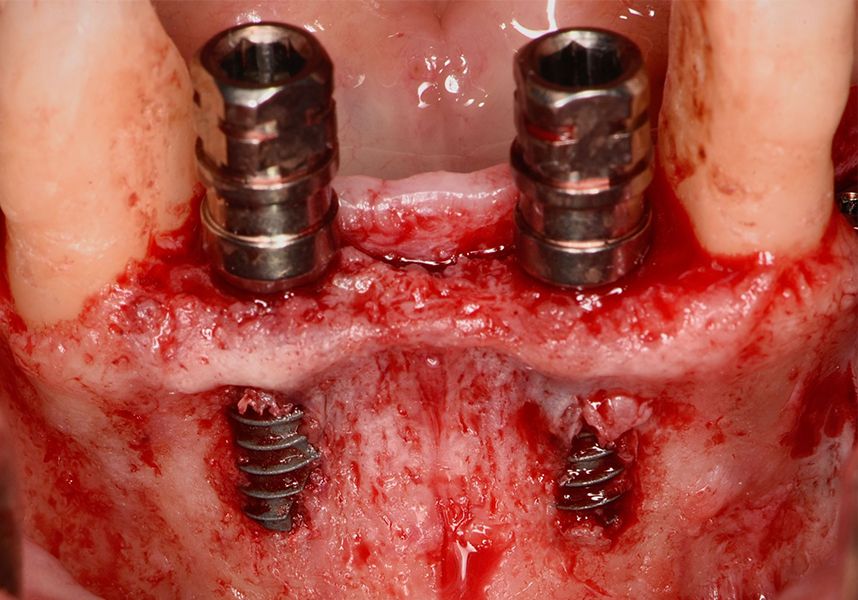
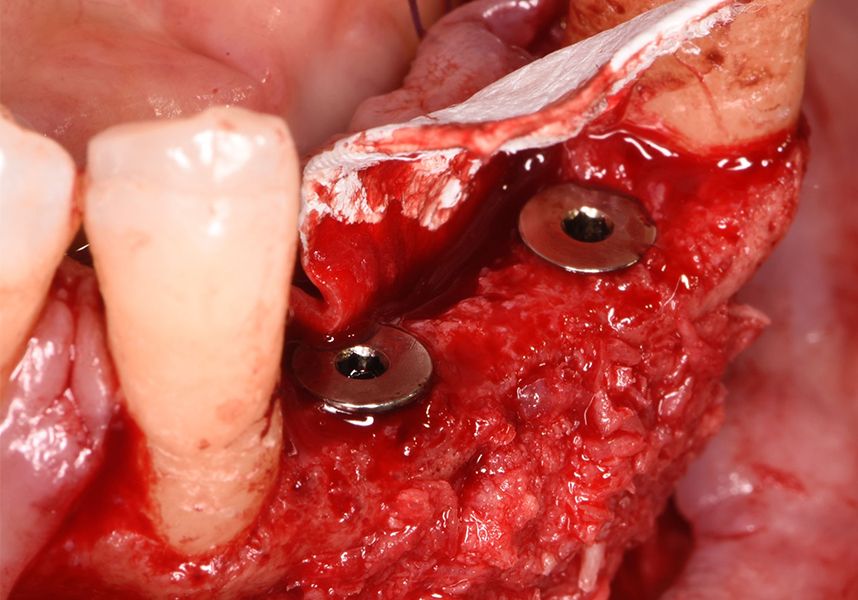
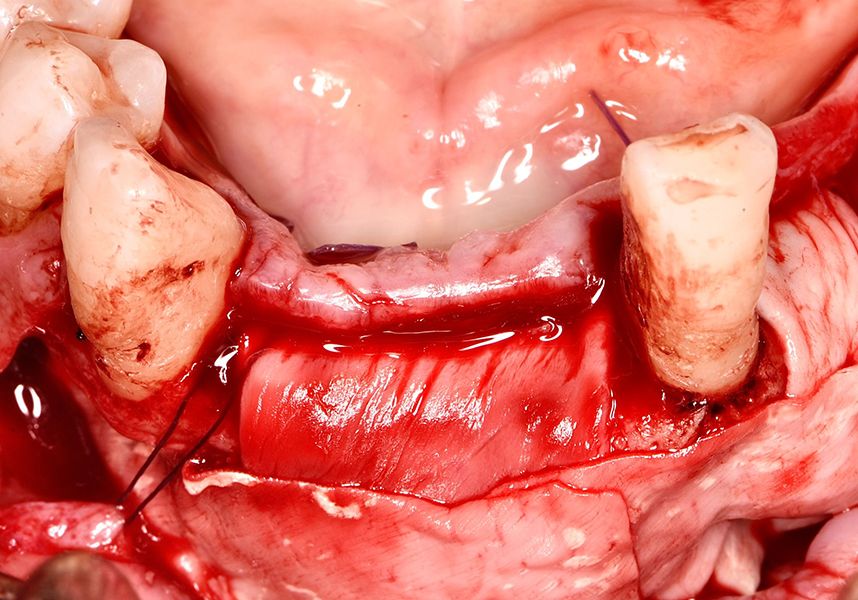
The patient was anesthetized and a flap was made from the distal area of tooth 43 up to 36. Then two Avinent Biomimetic Ocean IC implants of 3.5x10 were inserted in positions 32 and 42.
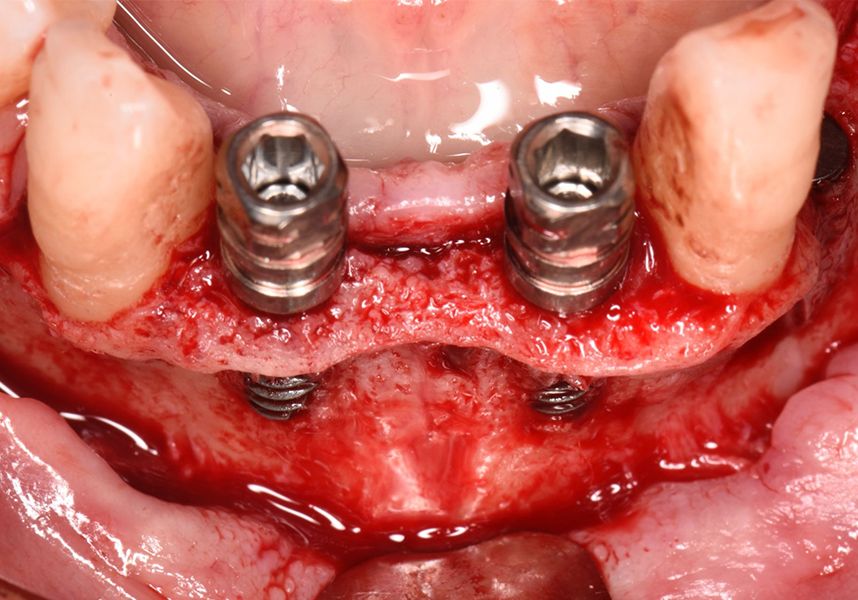
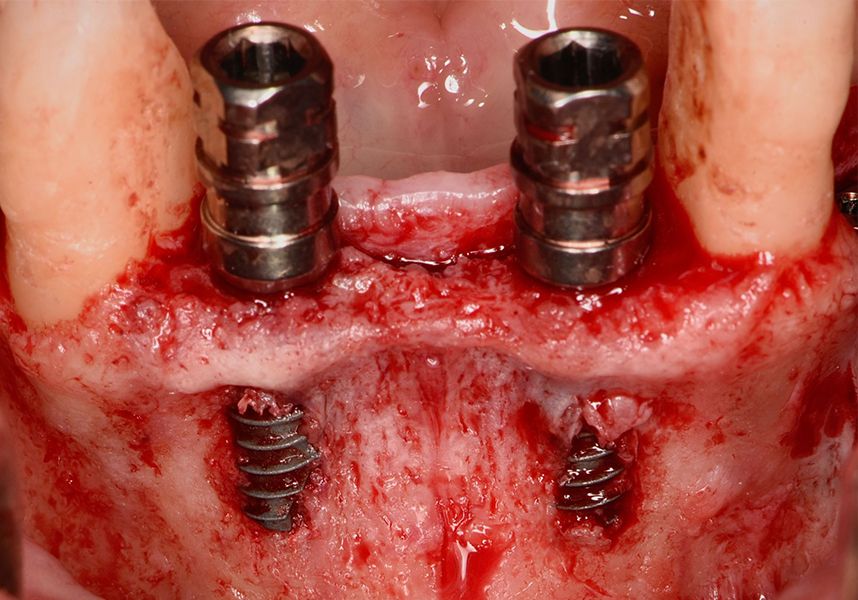
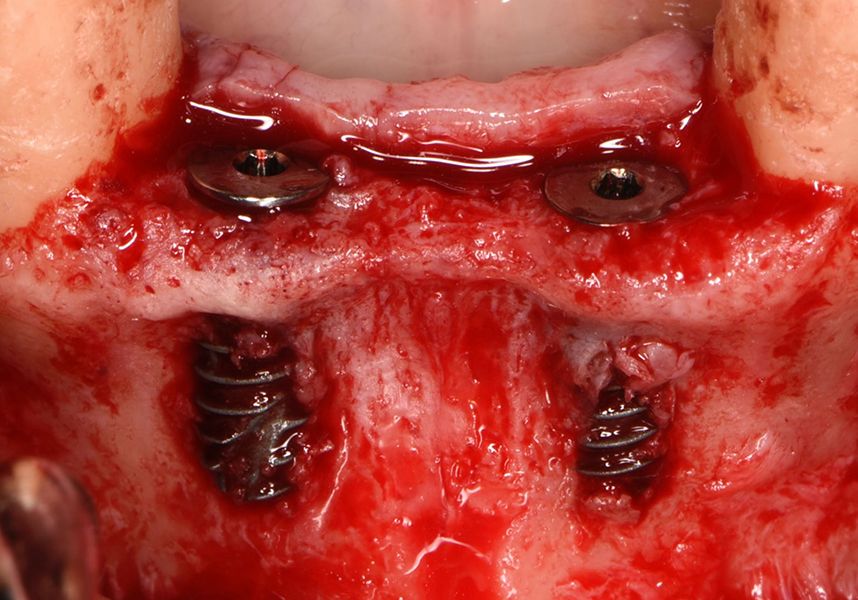
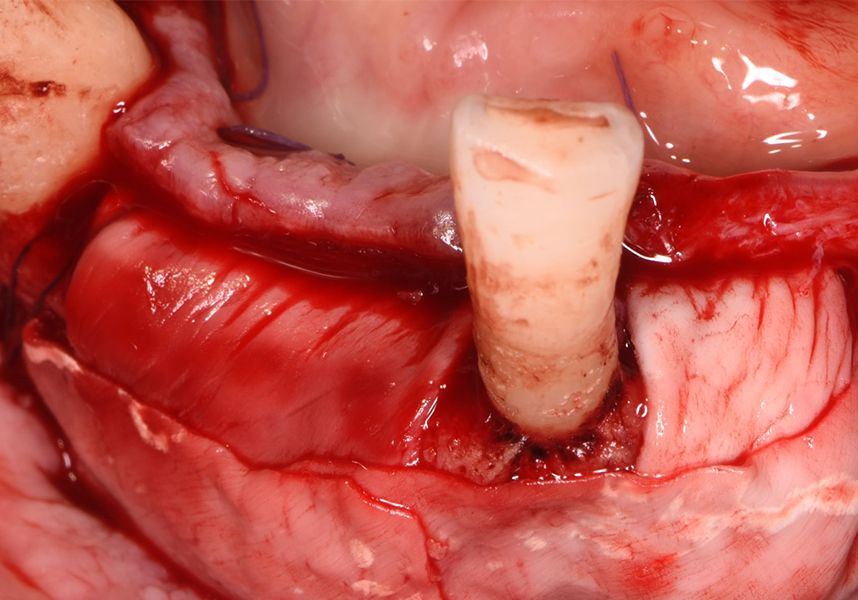
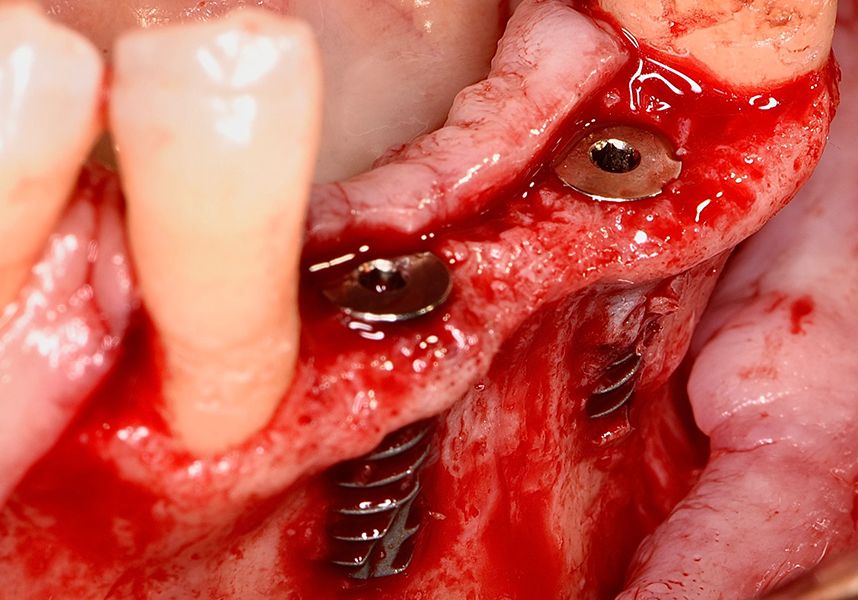
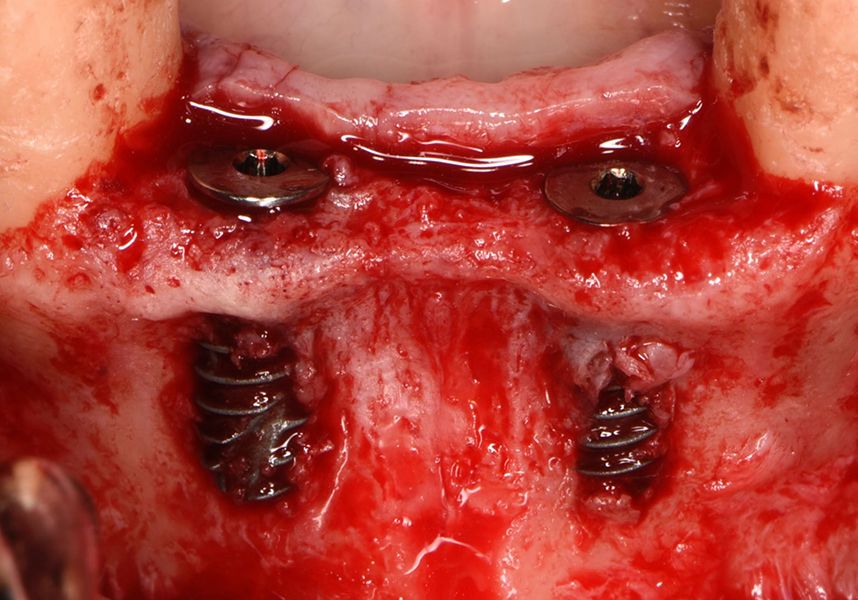
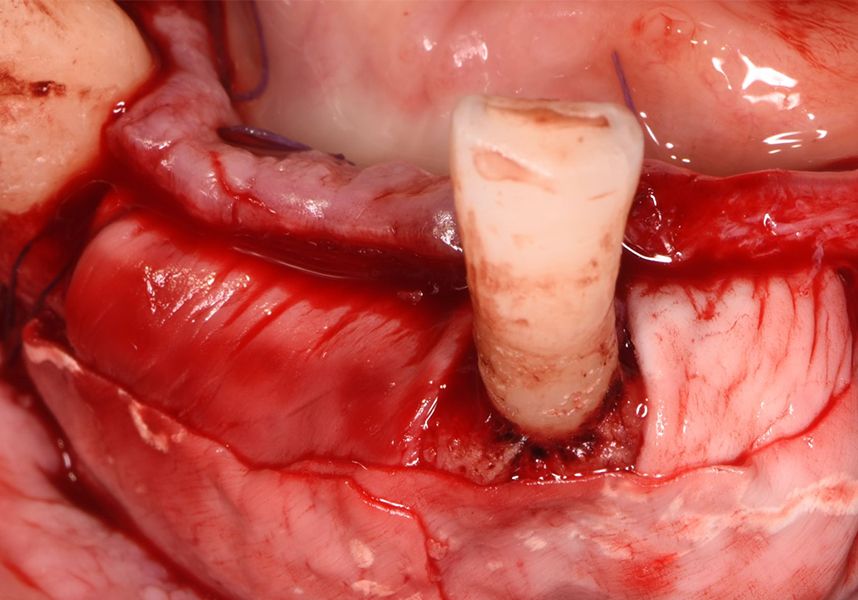
Respecting the three-dimensionally correct position of the implant led to bone fenestration, leaving the apical part of the apex of the implant exposed almost to the mid-point of its length at 42 and a third in 32.
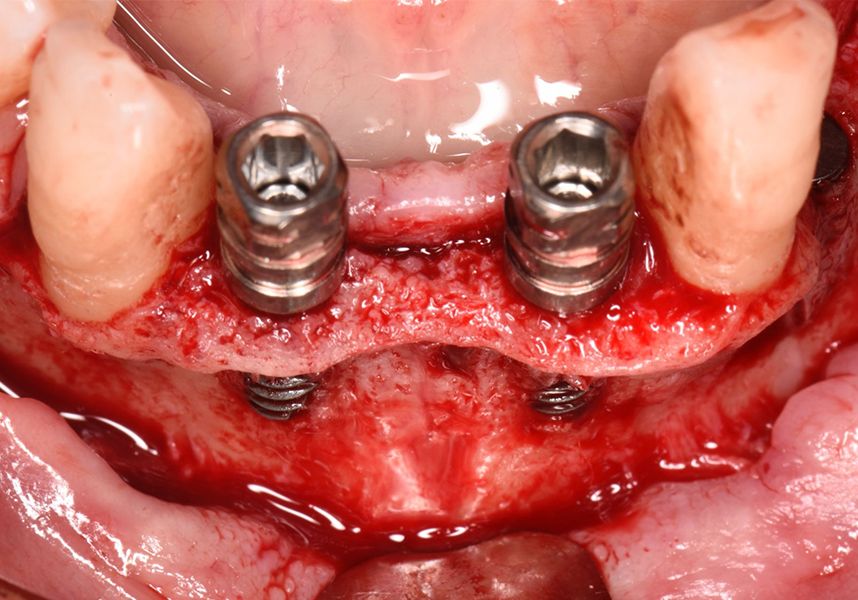
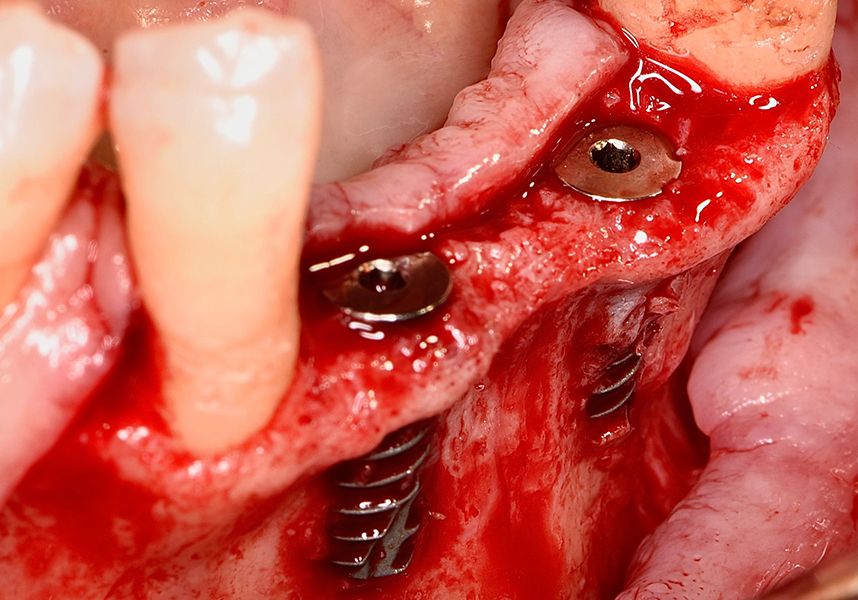
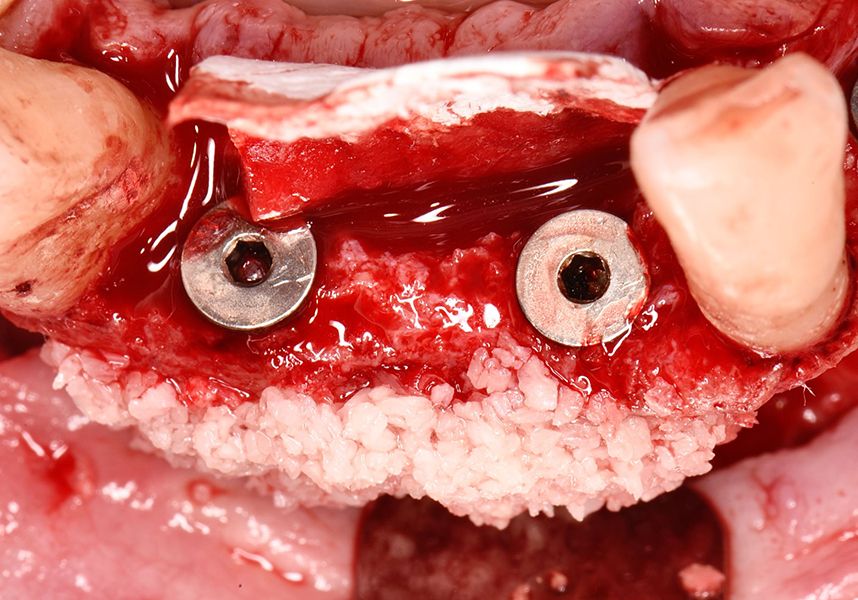
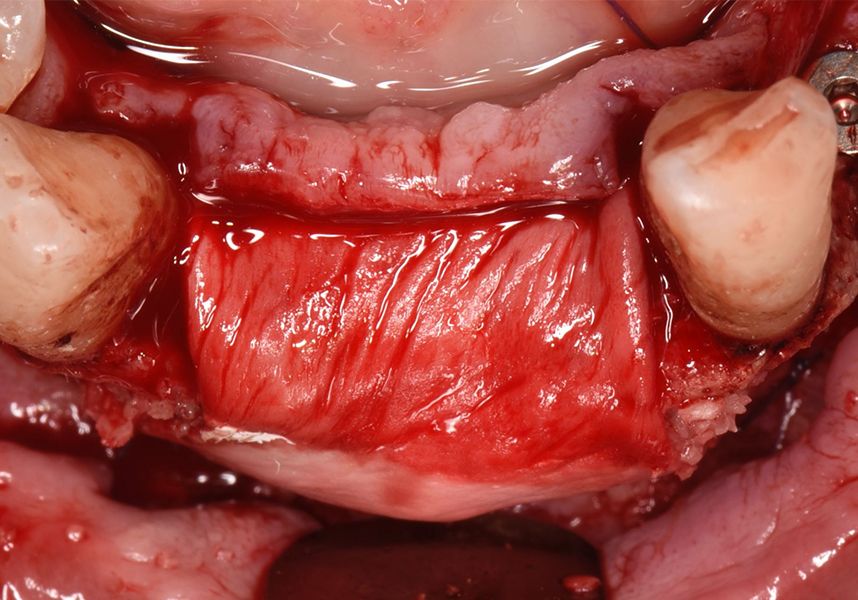
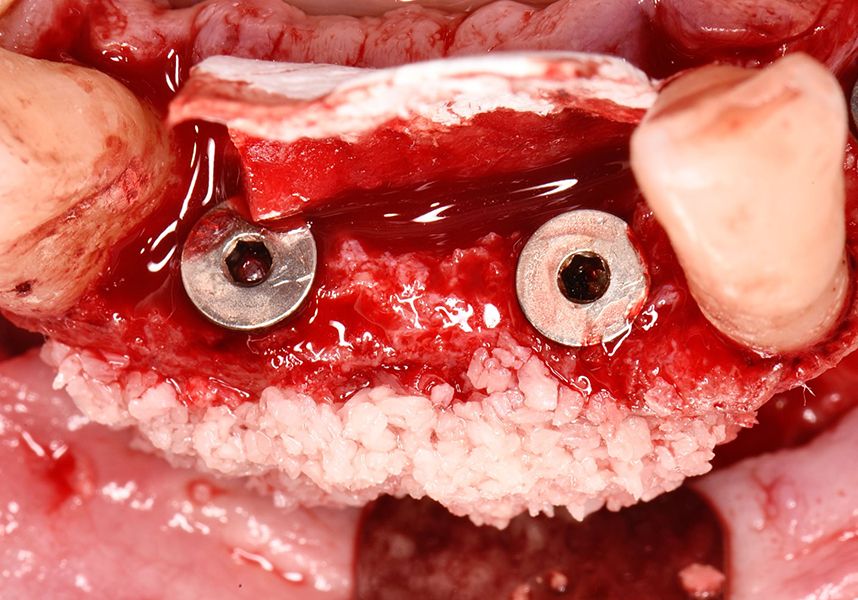
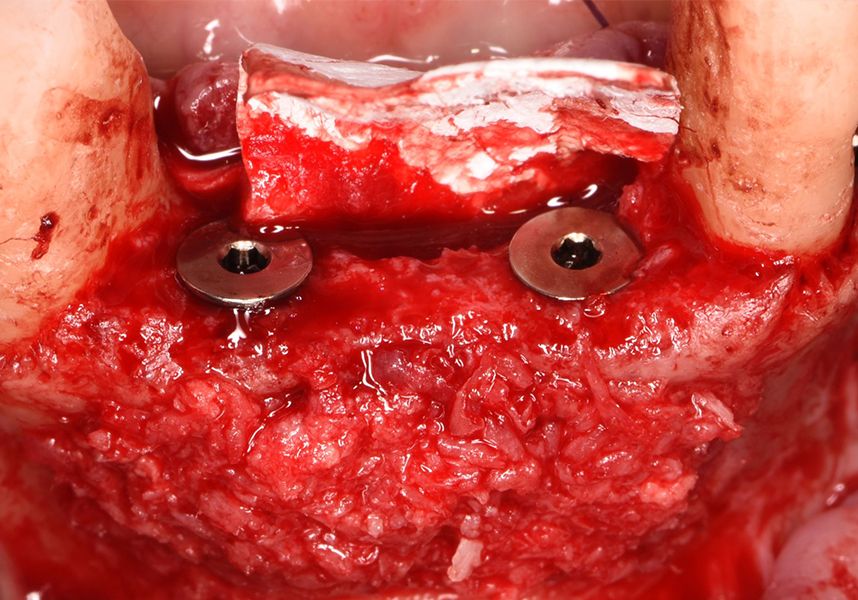
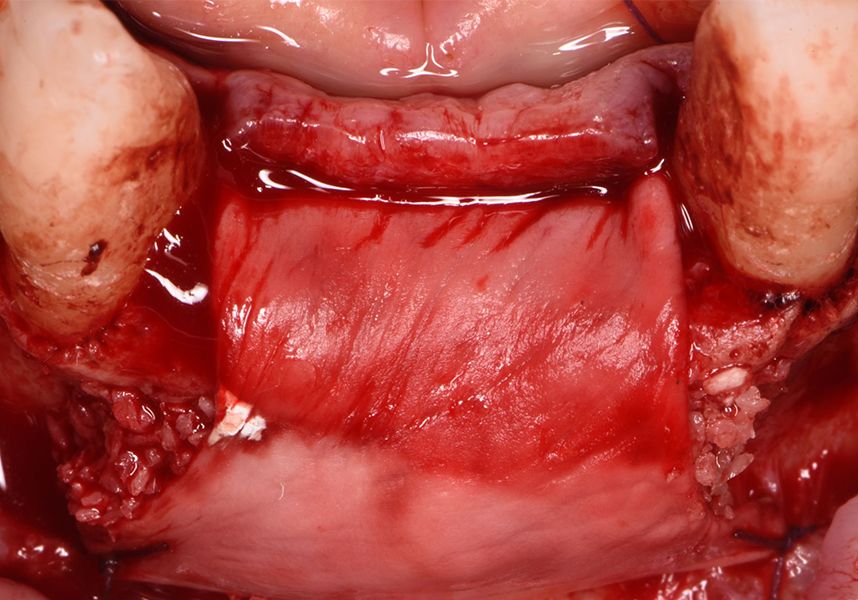
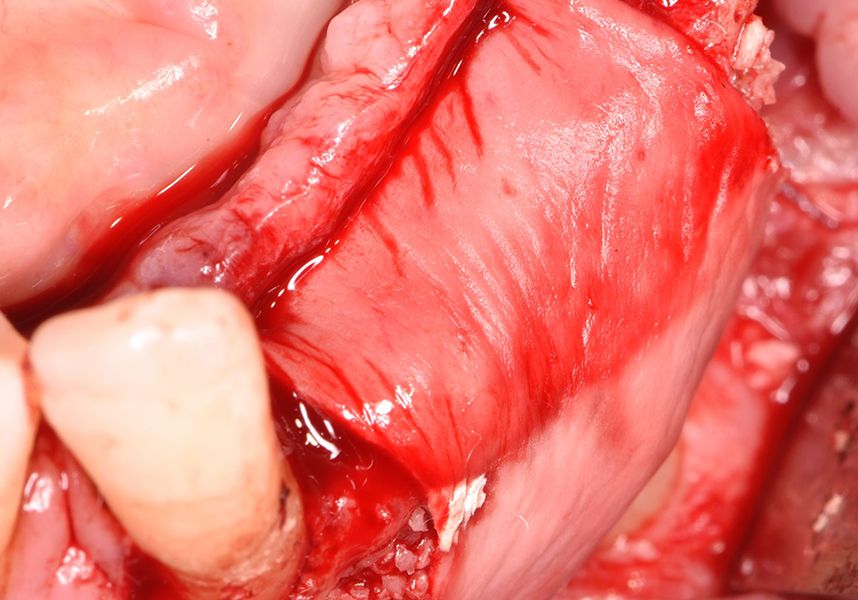
To treat the defect, bone regeneration was carried out simultaneous to the surgical process, with an autologous bone graft from the patient. In the internal part of the graft we used autologous cortical bone obtained by scraping (Safescraper) and from the biological drilling, at low revolutions and without irrigation, from the other implant beds. In the external layer of the regeneration we used a xenograft (Genoss, Osteogenos) and this was covered with a reabsorbable collagen barrier membrane (Evolution STD, Osteogenos).
The membrane was sutured with PGA reabsorbable suture to the periosteum to secure it, thus avoiding subsequent reentry to remove fixings such as tacks.


In the posterior sector three Biomimetic Ocean IC implants of 4.0x10 were inserted in positions 36, 34 and 46 with delayed load. A small regeneration was also carried out with autologous bone in the implant in position 34, where there was no exposure, but the vestibular cortical was very fine after implant insertion.
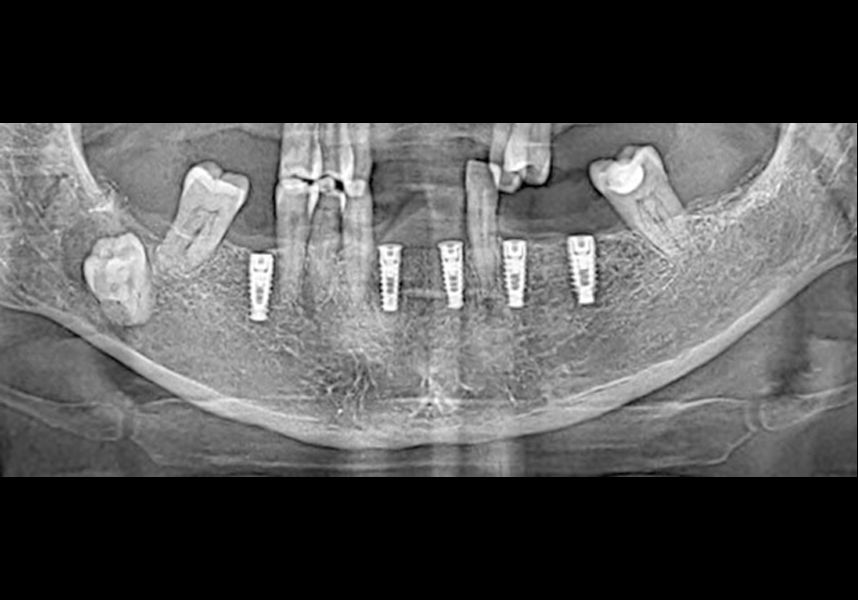
After a post-operative period without complications, the healing abutments were fitted in a second surgical stage 5 months later. Six months after implant placement, the final metal-ceramic prosthetic restoration was loaded.

Dental implants are currently a widely accepted therapeutic alternative when replacing lost teeth. However, like all therapeutic alternatives, they are not risk-free and require a number of conditions to be met to ensure the long-term success of the treatment.
It is essential to have enough bone tissue to be able to place the implants in the right position in the space depending on the prosthetic restoration planned. To do so, treatment with bone regeneration simultaneous to implant placement is often required, which is considered a predictable technique in minor defects such as dehiscence and fenestrations.