



Hi! - ENG




Ver evolución gráfica del caso
One of the most frequent complications of implant-supported prostheses, and which causes most visits to the surgery, is the loosening of the component that is screwed to the implant (1,2). Although, on most occasions it is simple to resolve (re-screw it to the torque recommended by the manufacturer), if this situation remains over time, the instability of the implant/attachment (or implant prosthesis, in this case of prostheses screwed to the implant head) and the unfavourable distribution of forces could end up causing the joining screw or screwed attachment (3) to fracture.
Although the clinic should warn the patient that mobility of an implant-supported prosthesis needs treatment and they should go to the surgery, it is often not until the prosthesis has completely de-inserted that the patient decides to request dental care and the fracture of the screw is detected (4). At this time, a part of the thread of the fractured screw or attachment is found in the de-inserted portion, but a fragment will remain inside the implant.
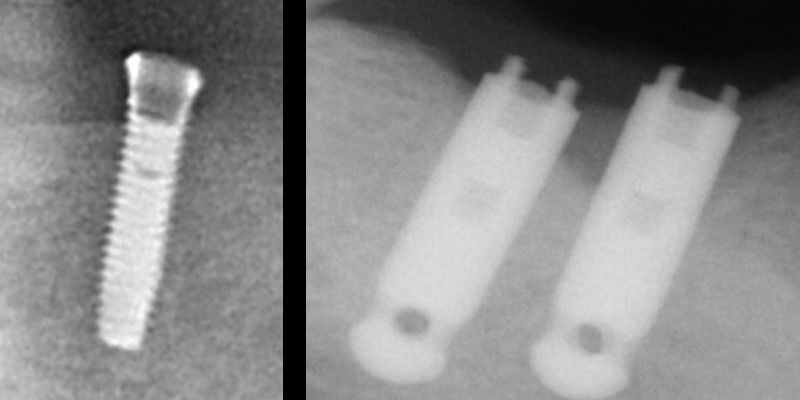
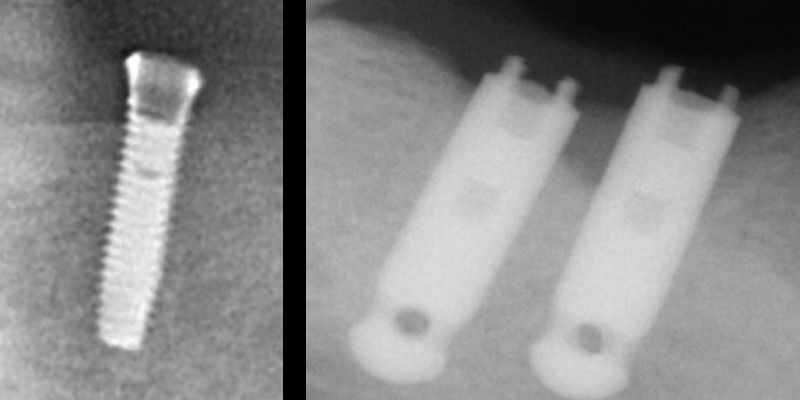
Detection of the fracture of the screw or screwed element can be simple by visual inspection of connection of the implant and the de-inserted part of the assembly, but often requires verification by tactile sensation with an instrument (e.g. exploratory probe) or the viewing of the fragment in a periapical x-ray. If there is an intact screw of the same system, it is also possible to compare with the fragment of extracted screw to determine if it is complete or not, or try to screw it to the implant body to check if there is any obstacle preventing it from being completely screwed on (4,5).
If
the situation of loosening or de-insertion of the prosthesis has remained over
time, the overgrowth of gingival tissue may hinder diagnosis. In this
case, to re-expose the implant platform and make
exploration easier, the method of choice will be the use of diode laser to
eliminate the excess tissue, since the use of an electric scalpel could transmit
excessive heat to the implant and the underlying bone, and the conventional
scalpel could scratch the implant’s outer surface, favouring its later
colonisation by microorganisms (5).

Once the presence of a fragment has been verified inside the implant, the main objective is to remove it to be able to screw in a new element. To do this, it needs to be rotated in the opposite direction to the screwing so that it slides along the internal thread of the implant to the exterior. That process is, on occasions, very quick and simple and, on others, requires more complex techniques, a greater consultation time or the case may even arise where it is not possible to successfully perform it, maintaining the integrity of the implant thread. In this last case, it would be necessary to explant the implant and replace it, or look for prosthodontic alternatives that do not require the use of the damaged implant (8,9).
Despite it being possible to find a large variety of cases of fractures with different fragment extraction techniques and some in vitro studies testing certain extraction methods in the literature, at today’s date there is no system or protocol available to act in the event of this complication.
According to Mizumoto et al. (5), we can classify the different available techniques in accordance with the difficulty and risk they entail for integrity of the implant and prosthesis. Using said classification, some of the techniques described in the literature are detailed below:
This category includes the most conservative methods performed with typically used instruments available in any dentist’s surgery.
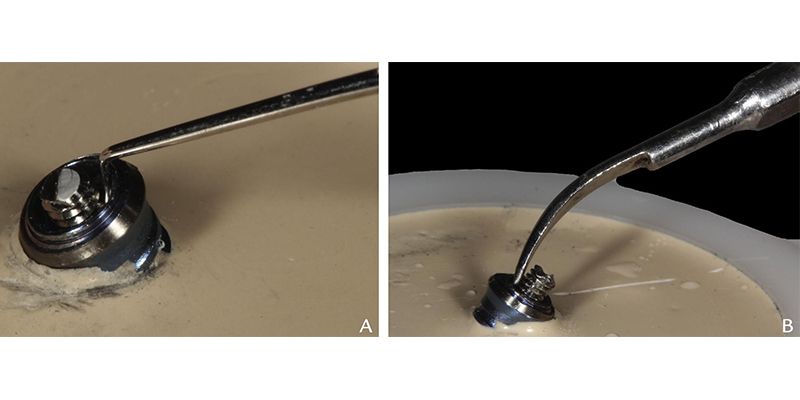
Using a fine, small and rigid instrument (exploratory or endodontic probe, curette) the tip is positioned on the coronal surface of the screw fragment and an anticlockwise movement is performed (4,5,8,10). Special care should be taken with very fine or flexible instruments such as, for example, endodontic files, that could fracture (11).

If these methods are not effective and the fragment moves from its place, vibration by the use of ultrasound may loosen it (5,7,10,12,13). It should be performed with a fine tip, a high power and applying a gentle rotation in anticlockwise direction on the occlusal surface of the screw to try to avoid vibration from inserting the screw deeper in the implant thread. It is recommendable to use abundant irrigation in order to not transmit high temperatures to the implant and surrounding bone (12,14).
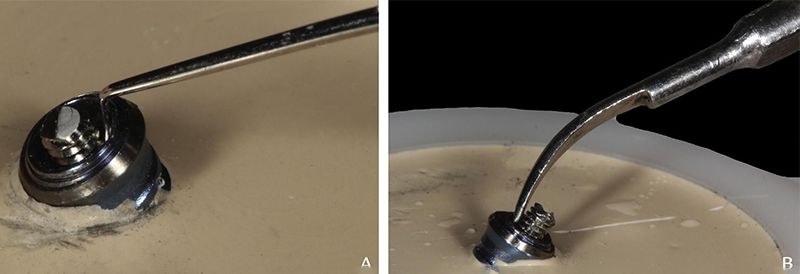
There are cases where despite the fragment having loosened, it is not simple to completely remove it from the implant thread: residues and deformations of the screw threads and of the implant may hinder the full sliding of the fragment to the exterior (7). In these cases, it is possible to use tweezers (13,16), needle-holders (3), cottons swabs (17), adhesive micro-applicators for restorations (16) to perform the complete extraction of the fragment.
Despite the fact that these techniques are considered low risk for the implant, special precautions should be taken in the use of the instruments, with the aim of avoiding damage, scratching or fracturing the internal threads of the implant (5).



This group includes the methods that require some modification to the screw fragment.
In the cases that the anchoring of the conservative instruments is not possible, a groove or notch that allows locking the instrument and exerting the rotation force may be of practical use (10,18–20). A transversal groove can be made to try to extract with fragment with the aid of a flat screwdriver, if there is one in the clinic, or this could even be made with the stem of a bur for straight handpiece, metal cutting discs and self-hardening acrylic handle (21).
If it was not possible to rotate the fragment manually, the use of the rotary instruments may be of use. It is performed by resting a bur, drill or trephine (the active part of which may be modified to make anchoring easier) on the fragment and actuating the rotary instrument in anticlockwise direction and at low speed (around 600 rpm) (5,19,20,22,23). Or instead, it is possible to combine both techniques: first make the groove in the fragment and then apply the rotary instrument so that the rotation exerted is more effective (19,20,22–24).
Some companies offer broken screw extraction kits, combining a series of instruments especially designed for this purpose: Fragment Fork® (Astra Tech®; Dentsply Sirona), Rescue Kit Straumann® (Institut Straumann AG®), Rescue Instrument Nobel Biocare® (Nobel Biocare®), and Certain-Screw Removal Kit (Biomet 3i®), which are compatible with their own make of implants. Others such as Broken Screw Extraction Kit from Rhein 83® are universal and can be used with most market platforms. These kits include bur guides which adapt to the implant platform that minimise the damage caused by the burs to the implant’s internal thread.
Next, the components and systems of use of one of the most widely used kits, Broken Screw Extraction Kit from Rhein 83®, is detailed:
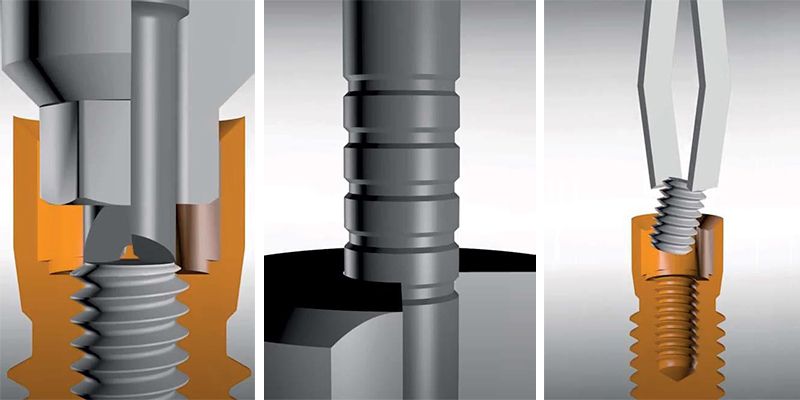
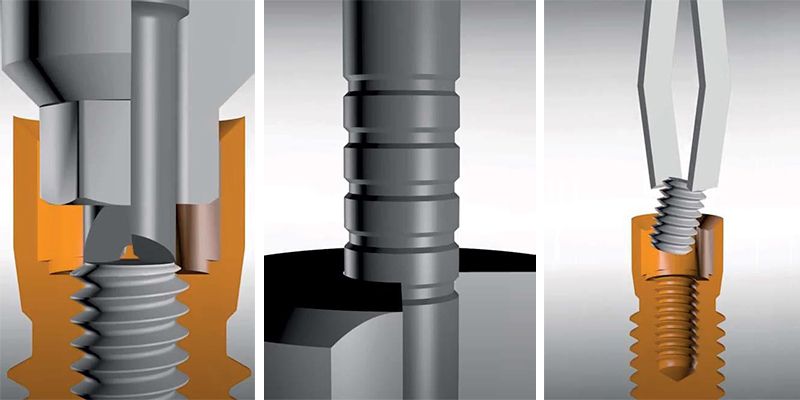
This kit is formed by a centring guide compatible with most market platforms, a “grip bur”, a “special bur” and a manual bur-holder device.

In first place, the manufacturer recommends starting with the “grip bur” manually applied. To do this we will place the centring guide on the implant platform and place in it the “grip bur” with the manual device. The active part of the “grip bur” is designed to facilitate gearing in the possible irregularities of the screw surface, hence manually applying an anticlockwise rotation it will be attempted to slide the screw towards the exterior. When all the notches of the bur stem are outside the centring guide, the screw will have been completely removed.

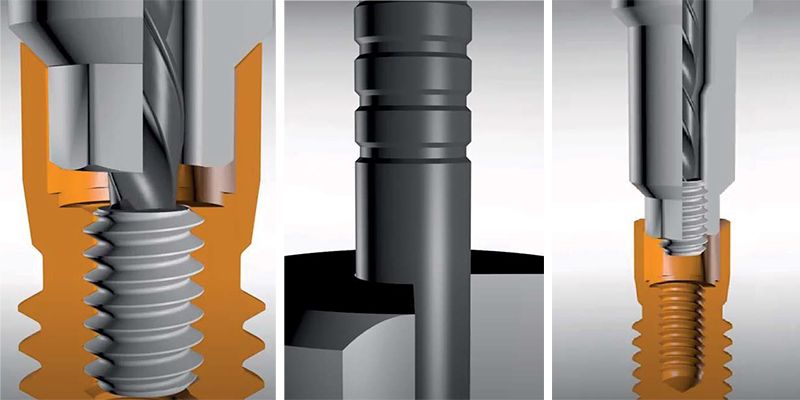
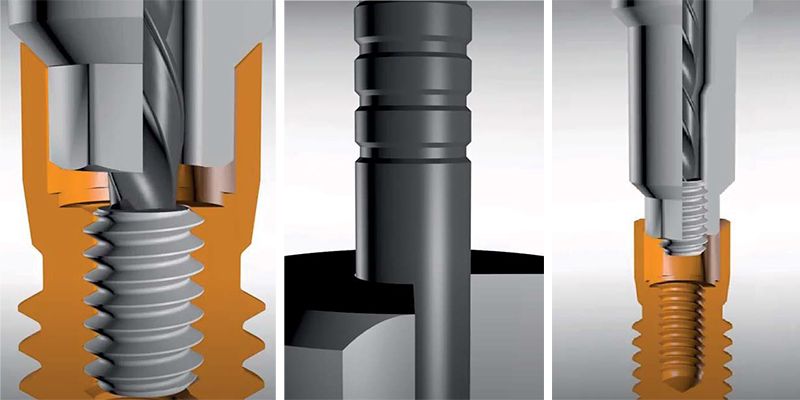
If the fragment remains blocked inside the implant, the next step is to attempt extraction with the “special bur” The centring guide shall also be used, and in the case, a counter angle of implantology shall also be used with anticlockwise rotation and maximum torque, applying constant pressure to prepare the fragment surface. The residues will be cleaned by applying water, air and suction in the internal implant chamber. Next, the “special bur” will be applied in anti-clockwise direction at a rate of between 500 and 600 rpm, using abundant irrigation for 3 seconds. In this way we can achieve either extraction or complete destruction of the screw.

The high-risk techniques are those that involve modification now not only of the screw, but also of the actual implant to be able to be used again for a new prosthesis.
They are divided into two groups: techniques that look to repair the implant thread to again enable the screwing of components and those that require complete elimination of the thread (5).
When the aforementioned methods for extracting screws have the unpleasant consequence of deformation of the implant’s internal thread, the contouring or reworking with manual or rotary instruments is an option that may simply resolve this problem (6,8,9,15,22,25–28).

Another technique consists of using these profilers when the fragment is still stuck inside the thread, paradoxically pushing it towards the inside of the implant, but making the thread more favourable for the later sliding of the screw in anticlockwise direction with any of the aforementioned instruments (6).
If the implant thread cannot be repaired with these methods, it is possible to not screw components in it and move on to a somewhat more aggressive technique: drill the internal thread of the implant completely, with diamond burs and abundant irrigation until it is completely smoothed, to later make a post & core using the conventional technique (29, 30).
If all the techniques fail, we should consider not using the problem implant despite being biologically healthy, leaving it buried in the mucosa and seeking another prosthodontic solution (5) or planning the explantation and placing of a new implant (8).
Bearing in mind this classification and the extraction methods described, even if there is no protocol or consensus in this regard, it seems sensible to start by the most conservative techniques and progressively increase the risk if the desired result is not obtained. The use of screw extraction kits can simplify the procedure, with specially designed instruments for a quick and effective extraction. The knowledge of these techniques by the clinic is highly convenient to avoid, insofar as is possible the need for surgical techniques that increase the biological and financial cost for the patient.
Article based on Gómez Prieto E, from Río Highsmith J. Análisis in vitro de la influencia de la deformación y reparación de la rosca interna del implante en el mantenimiento la precarga. Estudio piloto [Trabajo Fin de Máster]. (In vitro analysis of the influence of the deformation and repair of the internal screw of the implant in maintaining the preload.Pilot Study [Master’s Dissertation]). Madrid; Complutense University of Madrid; 2022








Bibliography
1.Huang Y, Wang J. Mechanism of and factors associated with the loosening of the implant abutment screw: A review. Journal of esthetic and restorative dentistry : official publication of the American Academy of Esthetic Dentistry . [et al]. julio de 2019;31(4):338-45.
2. Zembic A, Kim S, Zwahlen M, Kelly JR. Systematic Review of the Survival Rate and Incidence of Biologic, Technical, and Esthetic Complications of Single Implant Abutments Supporting Fixed Prostheses. Int J Oral Maxillofac Implants. enero de 2014;29(Supplement):99-116.
3. Maalhagh-Fard A, Jacobs LC. Retrieval of a Stripped Abutment Screw: A Clinical Report. J Prosthet Dent. octubre de 2010;104(4):212-5.
4. Raju S, Nair VV, Karunakaran HK, Manjuran NG. Management of perishing implants with abutment screw fracture - A systematic review. J Indian Prosthodont. septiembre de 2021;21(3):229-39.
5. Mizumoto RM, Jamjoom FZ, Yilmaz B. A risk-based decision making tree for managing fractured abutment and prosthetic screws: A systematic review. J Prosthet Dent. abril de 2018;119(4):552-9.
6. Imam AY, Moshaverinia A, Chee WWL, McGlumphy EA. A technique for retrieving fractured implant screws. J Prosthet Dent. enero de 2014;111(1):81-3.
7. Leblebicioğlu Kurtuluş İ, Emel K, Canakci FG. Scanning Electron Microscopic Analysis of the Screw Threads of Loosened and Fractured Abutments: A Case Report. Journal of Clinical and Diagnostic Research. 1 de marzo de 2018;12:ZD04-6.
8. Prado Naves Carneiro T de A, Prudente MS, Sales e Pessoa R, Mendonca G, das Neves FD. A conservative approach to retrieve a fractured abutment screw - Case report. J Prosthodont Res. abril de 2016;60(2):138-42.
9. Sprenger A, Gutauskas K, Filippi A, Rosentritt M, Kühl S. Stability of ImplantAbutment Connection After Using the Rescue Kit: An In Vitro Study. Int J Oral Maxillofac Implants. 12 de junio de 2018.
10. Joshi A, Kale VT, Suragimath G, Zope SA. An unconventional approach for retrieval of fractured prosthetic screw: A case report. J Osseointegration. septiembre de 2018;10(3):75-8.
11. Satterthwaite J, Rickman L. Retrieval of a fractured abutment screw thread from an implant: a case report. Br Dent J. 23 de febrero de 2008;204(4):177-80.
12. Bhandari S, Aggarwal N, Bakshi S. Ultrasonic Oscillations for Conservative Retrieval of a Rare Fracture of Implant Healing Abutment. J Oral Implant. agosto de 2013;39(4):475-8.
13. Al-Rawee RY, Mohammad FA, Tawfeeq BA. Salvage of fractured abutment screw by transfer cap screw replacement (original study). Clin Case Rep. junio de 2019;7(6):1204-10.
14. Igarashi K, Afrashtehfar K, Schimmel M, Gazzaz A, Brägger U. Performance of a Repair Service Set for the Retrieval of Fractured Abutment Screws: A Pilot In Vitro Study. The International journal of oral & maxillofacial implants. 10 de mayo de 2019;34.
15. Agustin-Panadero R, Baixauli-Lopez M, Gomez-Polo M, Cabanes-Gumbau G, Senent-Vicente G, Roig-Vanaclocha A. In vitro comparison of the efficacy of two fractured implant-prosthesis screw extraction methods: Conventional versus mechanical. J Prosthet Dent. diciembre de 2020;124(6):720-6.
16. Chen JH, Cho SH. An accessory technique for the intraoral removal of a fractured implant abutment screw. J Prosthet Dent. diciembre de 2018;120(6):812-5.
17. Barbosa JM, Ascenso J, Hirata R, Caramês J. The cotton driver: An alternative technique for removing fractured screw fragments. Journal of Prosthetic Dentistry. 1 de diciembre de 2014;112(6):1601-2.
18. Walia MS, Arora S, Luthra R, Walia PK. Removal of fractured dental implant screw using a new technique: a case report. J Oral Implantol. diciembre de 2012;38(6):747-50.
19. Williamson RT, Robinson FG. Retrieval technique for fractured implant screws. Journal of Prosthetic Dentistry. 1 de noviembre de 2001;86(5):549-50.
20. Gooty JR, Palakuru SK, Guntakalla VR, Nera M. Noninvasive method for retrieval of broken dental implant abutment screw. Contemp Clin Dent. abril de 2014;5(2):264- 7.
21. Kurt M, Guler AU, Duran I. A Technique for Removal of a Fractured Implant Abutment Screw. J Oral Implant. diciembre de 2013;39(6):723-6.
22. Taira Y, Sawase T. A Modified Technique for Removing a Failed Abutment Screw From an Implant With a Custom Guide Tube. J Oral Implant. abril de 2012;38(2):165-9.
23. Yoon JH, Lee H, Kim MY. Safe Removal of a Broken Abutment Screw with Customized Drill Guide and Rotary Instrument: A Clinical Report. Journal of prosthodontics : official journal of the American College of Prosthodontists. 2016;
24. Nergiz I, Schmage P, Shahin R. Removal of a fractured implant abutment screw: A clinical report. J Prosthet Dent. junio de 2004;91(6):513-7.
25. Luterbacher S, Fourmousis I, Lang NP, Brägger U. Fractured prosthetic abutments in osseointegrated implants: a technical complication to cope with. Clin Oral Implants Res. abril de 2000;11(2):163-70.
26. Joda T, Brägger U. Management of a complication with a fractured zirconia implant abutment in the esthetic zone. Int J Oral Maxillofac Implants. febrero de 2015;30(1):e21-23.
27. Lee JH, Park JH, Park CJ, Cho LR. Technique to retrieve implant abutment fragments. J Prosthet Dent. octubre de 2015;114(4):486-9.
28. Imam AY, Yilmaz B, Ozcelik TB, McGlumphy E. Salvaging an Angled Implant Abutment with Damaged Internal Threads: A Clinical Report. J Prosthet Dent. mayo de 2013;109(5):287-90.
29. Shah K, Lee DJ. An alternative approach for the management of fractured implant abutment screws on a mandibular implant-retained overdenture: A clinical report. J Prosthet Dent. abril de 2016;115(4):402-5.
30. Canpolat C, Ozkurt-Kayahan Z, Kazazoglu E. Management of a Fractured Implant Abutment Screw: A Clinical Report. J Prosthodont. julio de 2014;23(5):402-5.